Holistic Solutions Practice, PLLC D.B.A Life Coach Round Rock
Angela Hayes, MS, LMFT, Master Certified Life Coach
NOTICE OF GOOD FAITH ESTIMATE
THIS NOTICE DESCRIBES YOUR RIGHTS WITH REGARDS TO THE ‘NO SURPRISES ACT’ AS IT APPLIES TO PSYCHOTHERAPY. PLEASE REVIEW IT CAREFULLY.
Good Faith Estimate
You have the right to receive a “Good Faith Estimate” explaining how much your medical care will cost.
Under the law, health care providers need to give patients who don’t have insurance or who are not using insurance an estimate of the bill for medical items and services.
● You have the right to receive a Good Faith Estimate for the total expected cost of any non-emergency items or services. This includes related costs like medical tests, prescription drugs, equipment, and hospital fees.
● Make sure your health care provider gives you a Good Faith Estimate in writing at least 1 business day before your medical service or item. You can also ask your health care provider, and any other provider you choose, for a Good Faith Estimate before you schedule an item or service.
● If you receive a bill that is at least $400 more than your Good Faith Estimate, you can dispute the bill.
● Make sure to save a copy or picture of your Good Faith Estimate. For questions or more information about your right to a Good Faith Estimate, visit www.cms.gov/nosurprises or call 800-985-3059.
Effective January 1, 2022, a ruling went into effect called the “No Surprises Act,” which requires mental health practitioners to provide a “Good Faith Estimate” (GFE) about out-of-network care to any patient who is uninsured or who is insured but does not plan to use their insurance benefits to pay for health care items and/ or services.
The Good Faith Estimate works to show the cost of items and services that are reasonably expected for your mental health care needs for an item or service. The estimate is based on information known at the time the estimate was created. The Good Faith Estimate does not include any unknown or unexpected costs that may arise during treatment.
You are entitled to receive this “Good Faith Estimate” of what the charges could be for psychotherapy services provided to you. While it is not possible for a psychotherapist to know, in advance, how many psychotherapy sessions may be necessary or appropriate for a given person upon the initiation of psychotherapy, this form provides an estimate of the cost of services provided. Your total cost of services will depend upon the number of psychotherapy sessions you attend, your individual circumstances, and the type and amount of services that are provided to you. This estimate is not a contract and does not obligate you to obtain any services from the provider(s) listed, nor does it include any services rendered to you that are not identified here. Your total cost of services will depend upon the number of psychotherapy sessions you attend, your individual circumstances, and the type and amount of services that are provided to you. This estimate is not a contract and does not obligate you to obtain any services from the provider(s) listed, nor does it include any services rendered to you that are not identified here.

Most Commonly Billed services
This Good Faith Estimate is not intended to serve as a recommendation for treatment or a prediction that you may need to attend a specified number of psychotherapy visits. The number of visits that are appropriate in your case, and the estimated cost for those services, depends on your needs and what you agree to in consultation with your therapist. You are entitled to disagree with any recommendations made to you concerning your treatment and you may discontinue treatment at any time.
GENERAL GOOD FAITH ESTIMATE
The fee for a traditional 60-minute psychotherapy session (in-person or via telehealth) is $150. Clients may attend one psychotherapy visit per week, but the frequency of psychotherapy visits that are appropriate in your case may be more or less than once per week, depending upon your individual needs and preferences. It is also important, when determining your total estimate, to take into consideration vacations, holidays, emergencies, and sick time.
You may project any potential future cost(s) by multiplying the session fee of $150 by the total number of sessions. This will result in your total estimated cost for mental health service(s).
For example, $150 session fee X 4 sessions =$600.
If you attend therapy for a longer period, your total estimated charges will increase according to the number of visits and length of treatment.
Good faith estimates are based on the information the clinician has available at this time and actual items, services, or charges may differ from this good faith estimate as treatment progresses. Here is a chart of typical fees for services the practice provides that will be in effect from January 1, 2023, until further notice. Please note that these fees are the same for both in-office services and telehealth services.
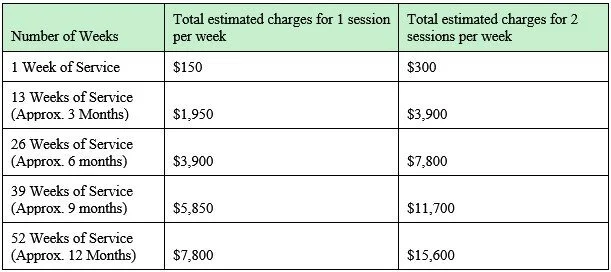
Good faith estimate per number of weeks of service
During the course of psychotherapy treatment, you may be subject to additional costs based on time, frequency, and services rendered. See below for a list of possible additional services:
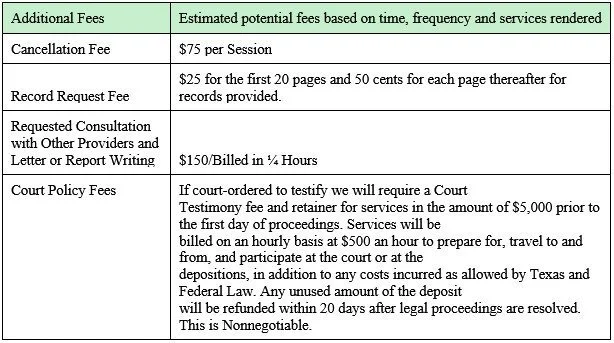
Additional fees
Life Coach Round Rock recognizes every client’s therapy journey is unique. How long you need to engage in therapy and how often you attend sessions will be influenced by many factors including:
● Your schedule and life circumstances
● Therapist availability
● Ongoing life challenges
● The nature of your specific challenges and how you address them
● Personal finances and resources
How many sessions you attend and how often are your decision and based on your unique needs and circumstances and can be changed at any time at your discretion. You and your therapist will continually assess the appropriate frequency of therapy and will work together to determine when you have met your goals and are ready for discharge and/ or a new “Good Faith Estimate” will be issued should the frequency of session(s) or needs change. As related, you may request a new GFE at any time in writing during your treatment.
Good Faith Estimate Disclaimer:
This Good Faith Estimate shows the costs of items and services that are reasonably expected for your health care needs for an item or service. The estimate is based on information known at the time the estimate was created. Your provider may recommend additional services that are not reflected in this Good Faith Estimate.
The Good Faith Estimate is only an estimate—actual items/ service charges may differ. The Good Faith Estimate does not include any unknown or unanticipated costs that may arise and are not reasonably expected during treatment due to unforeseen events. You could be charged more if complications or special circumstances occur. Other potential items and/ or services associated with therapy charges may include but is not limited to no show/ late cancellation fee(s), record request(s), letter writing(s), legal fee(s)/ court attendance(s), professional collaboration(s), and in-between session supports). These potential items / services and associated fee(s) are discussed further within the “Therapy Consent, Policies, and Agreements” documentation and should these items / services be initiated a new Good Faith Estimate will be provided. The Good Faith Estimate does not obligate the client to obtain listed items or services.
The Good Faith Estimate does not include any unknown or unexpected costs that may arise during treatment. You could be charged more if complications or special circumstances occur. If this happens, and your bill is $400 or more for any provider or facility than your Good Faith Estimate for that provider or facility, federal law allows you to dispute the bill.
You are encouraged to speak with your provider at any time about any questions you may have regarding your treatment plan, or the information provided to you in this Good Faith Estimate. You may contact the health care provider or facility listed to let them know the billed charges are higher than the Good Faith Estimate. You can ask them to update the bill to match the Good Faith Estimate, ask to negotiate the bill, or ask if there is financial assistance available.
You may also start a dispute resolution process with the U.S. Department of Health and Human Services (HHS). If you choose to use the dispute resolution process, you must start the dispute process within 120 calendar days (about 4 months) of the date on the original bill.
If you dispute your bill, the provider or facility cannot move the bill for the disputed item or service into collection or threaten to do so, or if the bill has already moved into collection, the provider or facility has to cease collection efforts. The provider or facility must also suspend the accrual of any late fees on unpaid bill amounts until after the dispute resolution process has concluded. The provider or facility cannot take or threaten to take any retributive action against you for disputing your bill.
There is a $25 fee to use the dispute process. If the Selected Dispute Resolution (SDR) entity reviewing your dispute agrees with you, you will have to pay the price on this Good Faith Estimate, reduced by the $25 fee. If the SDR entity disagrees with you and agrees with the health care provider or facility, you will have to pay the higher amount.
To learn more and get a form to start the process, go to www.cms.gov/nosurprises/consumers or call 1-800-985-3059.
For questions or more information about your right to a Good Faith Estimate or the dispute process, visit www.cms.gov/nosurprises/consumers, email FederalPPDRQuestions@cms.hhs.gov, or call 1-800-985-3059.
Keep a copy of this Good Faith Estimate in a safe place or take pictures of it. You may need it if you are billed a higher amount.
This notice first became effective on January 1st, 2023
512-843-2656
3000 Joe DiMaggio Blvd, Suite 1, Round Rock, TX 78665

ANGELA HAYES, MS,
LMFT, MASTER
CERTIFIED LIFE COACH